New Research in the Old Debate Over Spanking
Joan Lipuscek
Parent beliefs on the acceptability of spanking are often influenced by a wide variety of political, religious and cultural variables. Nevertheless, the overall attitude towards spanking in the U.S. has slowly been changing. According to the University of Chicago's General Social Survey, approximately 70% of U.S. parents currently indicate that spanking is an acceptable form of punishment compared to 84% in 1986 .
To add to the debate, last month a new meta-analysis entitled "Spanking and Child Outcomes: Old Controversies and New Meta-Analyses" by Gershoff and Grogan-Kaylor was published in the Journal of Family Psychology. The study "found no evidence that spanking is associated with improved child behavior and rather found spanking to be associated with increased risk of 13 detrimental outcomes." The study went on to recommend that "Parents who use spanking, practitioners who recommend it, and policymakers who allow it might reconsider doing so given that there is no evidence that spanking does any good for children and all evidence points to the risk of it doing harm."
This new analysis evaluated a total of 1,574 studies related to the use of spanking children as a disciplinary measure used by parents. Then, the list of studies was narrowed using the following criteria:
1) Studies had to be published in a peer-reviewed journal.
2) Studies had to include "a measure of parents' use of customary, noninjurious spanking (or slapping or hitting)" to insure that studies of physical abuse were not included.
3) Studies had to report an association between spanking and child outcomes.
4) Studies had to include "appropriate statistics for calculating effect sizes" (Cohen's d).
As a result of this criteria, the list of studies was narrowed to 75. These studies produced a total of 111 effect sizes that the researchers used for their analysis. The 111 effect sizes included data from 160,927 unique children. The oldest studies included in the analysis are from 1961, while the newest are from 2014. Thus, research from over five decades has been included.
We have created the following visualizations that summarize a portion of the findings from this study. (Please set your browser to allow third party cookies if you receive an error while trying to explore the data.)
Note: The calculations in the graphic are based on Cohen's d reported by outcome and study. Each Cohen's d is converted into a Number Needed to Treat using the Excel formula:
Number Needed to Treat = 1/(NORMSDIST(Cohen's d +NORMSINV(Control Event Rate))-Control Event Rate)
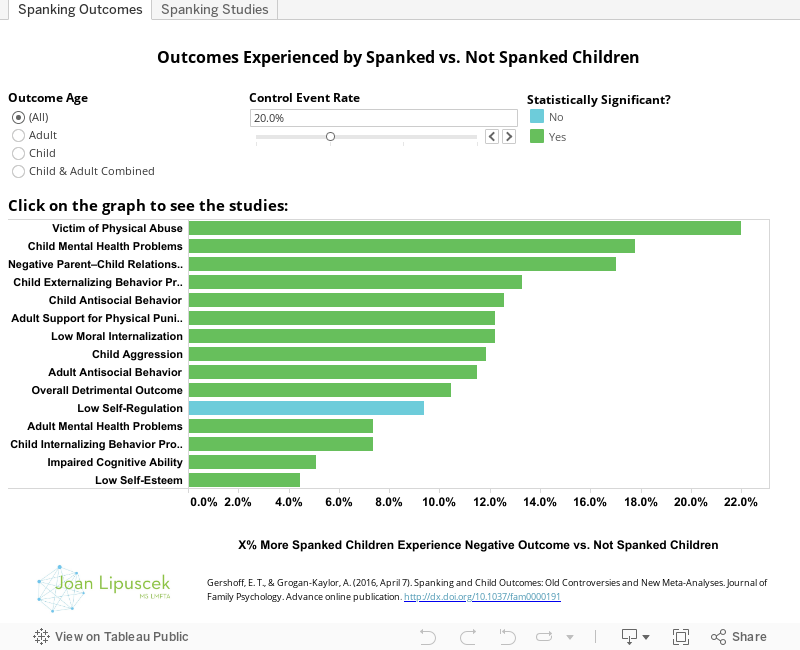
Because we do not know the exact rate of negative child and adult outcomes for children that were not spanked (Control Event Rate), we allow readers to change this variable from 10% to 40%. Then, we determine the % Increase of Negative Outcomes for Spanked Children Compared to Not Spanked Children using 1/Number Needed to Treat.
THE RESULTS
The first tab "Spanking Outcomes" lists 17 different negative psychological outcomes. The study found that spanked children experienced each negative outcome more than children who were not spanked. However, only 13 of the 17 negative outcomes showed a statistically significant increase among spanked children. Of these, 10 were child outcomes. Spanked children were at an increased risk of being a victim of physical abuse, having mental health problems, having a negative parent-child relationship, externalizing behavior problems, anti-social behavior, low moral internalization, aggression, internalizing behavior problems, impaired cognitive ability and low self-esteem. In addition, the study showed that spanked children are at an increased risk of negative adult outcomes including support for physical punishment of children, antisocial behavior and mental health problems.
The second tab "Spanking Studies" shows all the different studies that the researchers used to obtain these results. Positive results indicate that spanked children are at elevated risk for negative psychological outcomes. Negative results indicate that spanked children are at reduced risk for negative psychological outcomes.
Of all the studies that were included, 102 of the 111 effect sizes showed elevated risk of negative psychological outcomes for children that were spanked. Only nine studies showed reduced risk of negative psychological outcomes for children that were spanked and only one (Tennant, Detals, & Clark, 1975) was statistically significant.
COUNTER EVIDENCE
Professor Gershoff has long been associated with research on spanking and corporal punishment. Her 2002 study, "Corporal Punishment by Parents and Associated Child Behaviors and Experiences: A Meta-Analytic and Theoretical Review" is widely cited and critiqued using two primary arguments.
Argument #1: Professor Gershoff's 2002 study grouped spanking with other forms of more severe physical punishment. As a result, her 2002 study overstated the negative outcomes due to spanking. This line of argument was explored in "Ordinary Physical Punishment: Is It Harmful? Comment on Gershoff (2002)" by Baumrind et al. When this critique reanalyzed the sample used in Professor Gershoff's 2002 study, it found that negative child outcomes were more highly associated with severe forms of corporal punishment compared to less severe forms such as spanking.
Thus, this study concluded that "Because her [Professor Gershoff's] measure included many instances of extreme and excessive physical punishment, her analyses are not relevant to the current political debate about whether normative spanking...is harmful for children. At present we conclude that the evidence presented in Gershoff’s meta-analyses does not justify a blanket injunction against mild to moderate disciplinary spanking."
In their new paper, Professors Gershoff and Grogan-Kaylor respond to this critique by noting that these researchers "concluded that only severe methods of physical punishment are harmful." However, the professors note that this critique included statistics comparing more severe and less severe forms of corporal punishment that indicate "that both are associated with more undesirable child outcomes."
This critique led Professors Gershoff and Grogan-Kaylor to modify the criteria for a study's inclusion in their updated analysis. In their latest analysis, only studies that had "a measure of parents' use of customary, noninjurious spanking (or slapping or hitting)" were included to insure that studies of physical abuse were excluded (Criteria #2 for inclusion of a study described above).
Argument #2: Professor Gershoff's meta-analysis is relying on a sample of methodologically weak studies that have have not conducted randomized controlled experiments. However, as Professors Gershoff and Grogan-Kaylor note in their latest analysis, "parents' use of spanking is not easily or ethically studied through an experimental design, as children cannot be randomly assigned to parents with varying predispositions to spank, nor can parents typically be randomly assigned to spank or not spank."
Due to this problem, studies have not been able to "causally link spanking with child outcomes" because they suffer from "selection bias in who gets spanked - children with more behavior problems elicit more discipline generally and spanking in particular." This critique is covered in "The Intervention Selection Bias: An Underrecognized Confound in Intervention Research" by Larzelere et al.
In response, Professors Gershoff and Grogan-Kaylor note that analyses that have used advanced statistical methods to mitigate these concerns and focused only on the most methodologically sound studies have failed to find evidence that spanking produces positive child outcomes. Instead, studies such as "Spanking, corporal punishment and negative long-term outcomes: a meta-analytic review of longitudinal studies" by Ferguson have found "small but non-trivial long-term relationships between spanking/corporal punishment use and negative outcomes."
Advice for parents
As mentioned in the introduction, the decision to spank or not spank a child is deeply personal and the aim of this post is not to judge individual parenting decisions. However, it may be valuable for interested parents to understand the latest research and counter-arguments in this area of study.
In our review of the research, it appears reasonable to conclude the following:
1) There is little evidence to suggest that spanking leads to positive child outcomes.
2) At best, mild spanking adds little to no risk of negative child outcomes.
3) At worst, even mild spanking significantly increases risk of negative child and adult psychological outcomes.
With the evidence stacking up in favor of not spanking children, parents may want to question why they are continuing this practice. Would alternative forms of non-physical discipline prove as effective without the increased risk of negative psychological outcomes? Would brief "time-outs" or a short-term loss of privileges accomplish the same goals as spanking?
If trends on attitudes towards the acceptability of spanking continue, the practice of spanking is in no danger of a quick extinction. However, with new research and critiques working to improve methods and provide more sound conclusions, there appears to be mounting evidence that spanking is a practice that is ineffective at best and detrimental at worst.