Characteristics and Effects of Child & Teen Bullying
Joan Lipuscek
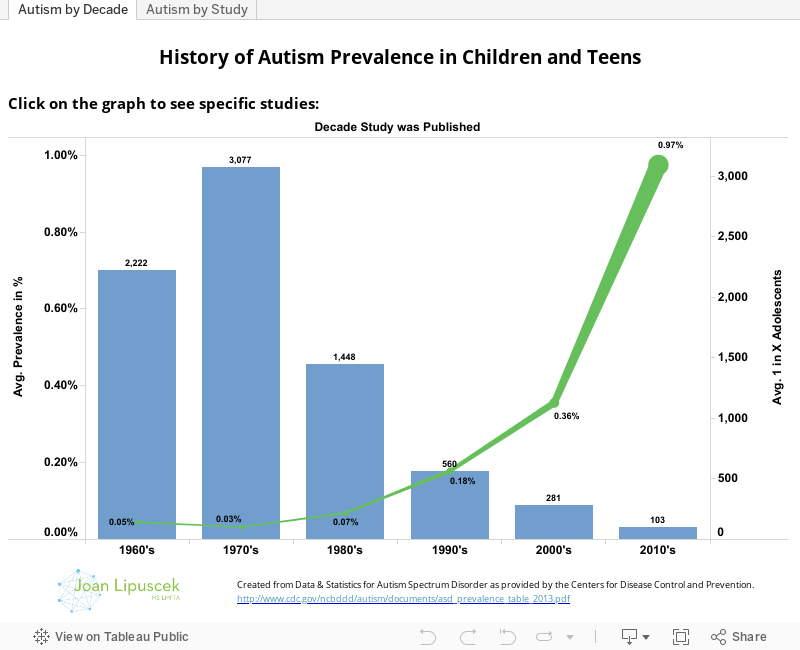
Research on bullying has become increasingly sophisticated and a growing number of mental health researchers are interested in the topic. In this post we present the results of the study Adult Psychiatric Outcomes of Bullying and Being Bullied by Peers in Childhood and Adolescence by Copeland et al. published in JAMA Psychiatry on 2/20/2013.
The data for this study is from the Great Smoky Mountain Study which assessed children and teens from ages 9-16 and followed them through ages 19-26. The series of visualizations that we have created attempts to summarize the study's findings into three primary questions. (Please set your browser to allow third party cookies if you receive an error while trying to explore the data.)
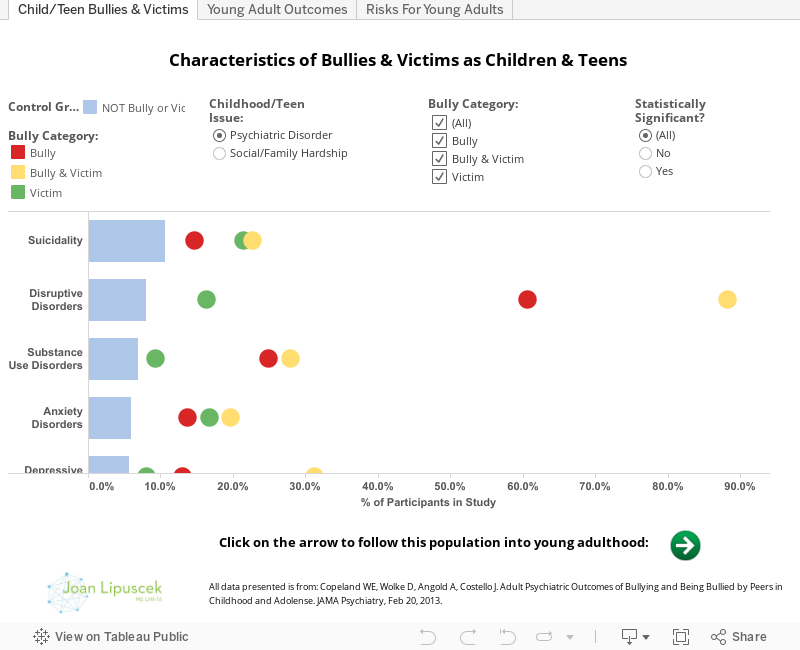
Question #1 (Visualization Tab - "Child/Teen Bullies & Victims") - What are the characteristics of children and teens who are victims of bullying, both bullies and victims, and bullies?
We begin with the characteristics of children and teens who were neither bullies nor victims. We report the prevalence of psychiatric disorders and social hardship for this group of children and teens in the blue bars. Then, we overlay the study's findings of these same psychiatric disorders and social hardships for children and teens that were identified as victims of bullying, both bullies and victims, and bullies. As shown on the visualization, the study found that child and teen victims, both bullies and victims, and bullies are significantly more likely to have a variety of psychiatric disorders and social hardship. These findings are consistent with earlier studies.
Question #2 (Visualization Tab - "Young Adult Outcomes") - What are the psychiatric characteristics of young adults that were victims, both bullies and victims, and bullies as children and teens?
As we follow the population into young adulthood, several trends emerge.
1) Bullies - First, child and teen bullies are at elevated risk for very few mental disorders as young adults. There is a statistically significant increase in risk for only antisocial personality disorder for child and teen bullies as young adults.
2) Victims - Young adults who were victimized as children and teens, on the other hand, showed significant increases in risk for a variety of mental disorders including agoraphobia, anxiety disorders, generalized anxiety, depressive disorders and panic disorders.
3) Bullies and Victims - Young adults that were both bullies and victims as children and teens show the most elevated risks for mental disorders as young adults. This group faces increased risk in both the breath and prevalence of mental disorders as young adults.
Question #3 (Visualization Tab - "Risks for Young Adults") - After controlling for psychiatric disorders and social hardships as a child and teen, how much does being a victim, bully and victim, and bully as a child and teen increase one's risk for psychiatric disorders as a young adult?
1) Bullies - Again, children and teens who were bullies show increased risk of only antisocial personality behavior as young adults.
2) Victims - After controlling for childhood and teen psychiatric disorders and social hardships, victims of bullying continue to show significant increased risk for agoraphobia, anxiety disorders, panic disorders and generalized anxiety as young adults. The increased risk for depressive disorders is no longer statistically significant after controlling for childhood and teen psychiatric disorders and social hardships.
3) Bullies and Victims - After controlling for childhood and teen psychiatric disorders and social hardships, bullies and victims continue to show significant increased risk for panic and depressive disorders. Interestingly, male bullies and victims show a very high increase in risk for suicidality as young adults, while females do not. Female bullies and victims show a very high increase in risk for agoraphobia as young adults, while males do not.
ADVICE FOR PARENTS
Childhood bullying should not be ignored or dismissed by parents or school administrators as a rite of passage. Instead, it is a serious issue that significantly increases risks for psychiatric disorders for childhood and teen victims, both victims and bullies, and bullies as they age and become young adults. Parents should take claims of bullying and victimization from children seriously and look to intervene by working with school administrators and teachers to stop the bullying behavior and prevent it from happening in the future.
The study "Effectiveness of School-Based Programs to Reduce Bullying: A Systematic and Meta-analytic Review" by Ttofi et al. was conducted to evaluate the effectiveness of school-based anti-bullying programs. The study found programs to be effective by decreasing bullying by 20-23% and victimization by 17-20% on average. In evaluating what makes school-based anti-bullying programs effective, the study found that, "More intensive programs were more effective, as were programs including parent meetings, firm disciplinary methods, and improved playground supervision." Parents of children and teens struggling with bullying behavior should ask their schools about their anti-bullying programs and raise awareness about the effectiveness of these programs in order to enact a positive change.
Note: To calculate the risk presented in the visualizations, we used the formula Relative Risk = Odds Ratio/((1 - p)+(Odds Ratio * p)) where p is the prevalence of psychiatric disorders in young adults that were not bullies or victims as children and teens.