
Youngest Children in Class at Greater Risk for ADHD Diagnosis & Medication
Joan Lipuscek
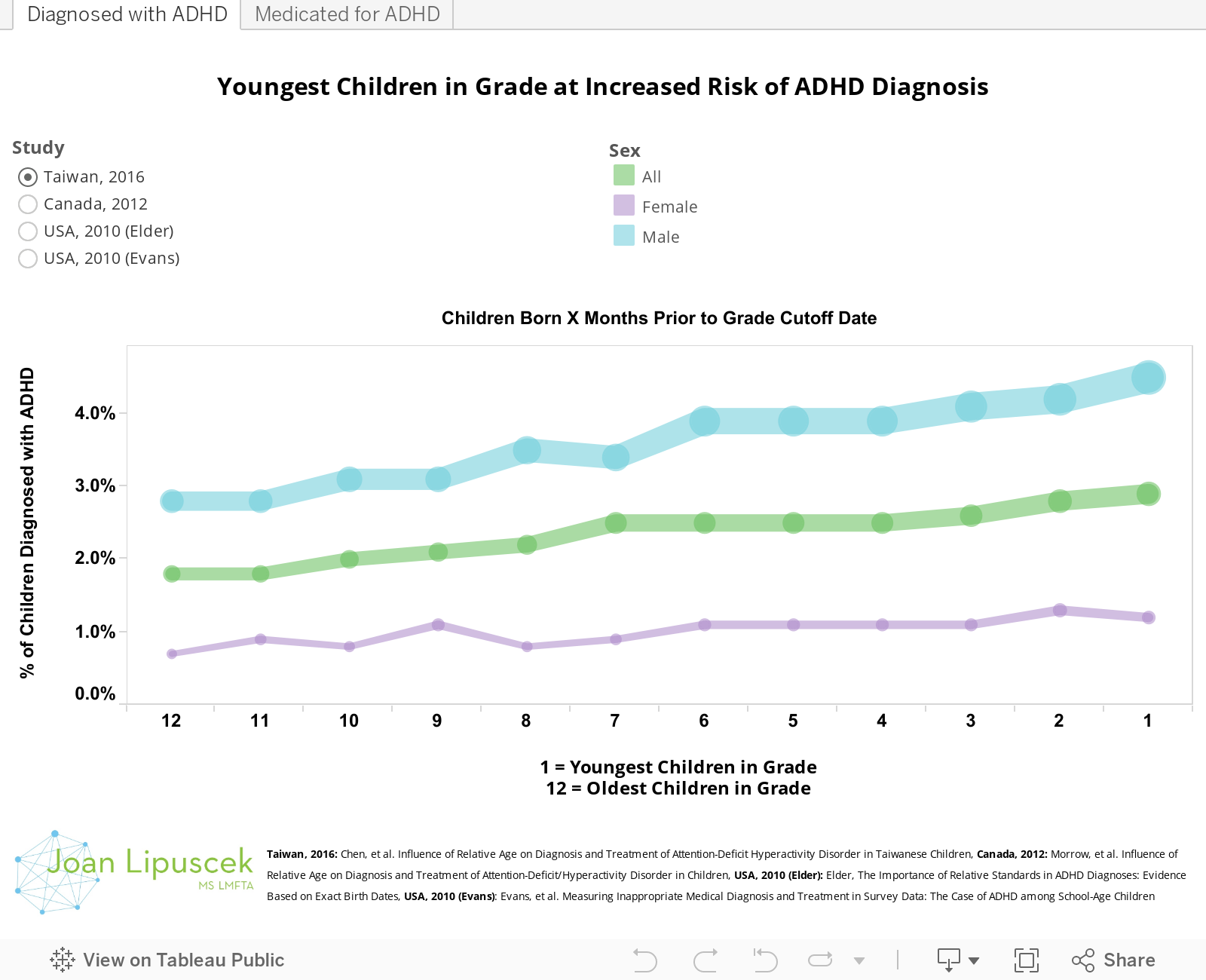
In March 2016, a new Taiwanese study was published in The Journal of Pediatrics that showed that the youngest children in a class are at greater risk of being diagnosed and medicated for ADHD compared to older classmates. The implication is that the youngest children in a class are overdiagnosed with ADHD due simply to immaturity.
The results of this study appear consistent with a number of other studies from around the world. The U.S., Canada, Iceland and now Taiwan have all produced studies that find that relative age in a classroom is a very important factor when diagnosing and medicating for ADHD.
Although countries and states have different cutoff dates for school children to enter a class, we adjusted the data for each study so that readers can easily see the trend of higher rates of ADHD diagnosis and medication for the youngest children in the class. (Please set your browser to allow third party cookies if you receive an error while trying to explore the data.)
THE STUDIES
Taiwan, 2016 - Chen, et al. "Influence of Relative Age on Diagnosis and Treatment of Attention-Deficit Hyperactivity Disorder in Taiwanese Children" This is the latest study on the importance of relative age in diagnosing ADHD. The sample was 378,881 Taiwanese school children ages 4-17 in school from 1997 to 2011. Kids born just one month prior to the grade cutoff date were 61% more likely to be diagnosed with ADHD compared to their oldest classmates. These youngest children were also 75% more likely to be medicated compared to their oldest classmates. Results were consistent for both boys and girls.
Canada, 2012 - Morrow, et al. "Influence of Relative Age on Diagnosis and Treatment of Attention-Deficit/Hyperactivity Disorder in Children" Consistent with the findings in Taiwan, this Canadian study also found a higher risk for the youngest boys and girls of a class being both diagnosed and medicated for ADHD. The sample was 937,943 children in British Columbia ranging between 6 and 12 years of age using data from the 11 years between 1997 through 2008. The study found that male children born one month prior to the grade cutoff date were 30% more likely to be diagnosed with ADHD and 41% more likely to be medicated compared to the oldest male children in the same grade. Female children born one month prior to the grade cutoff date were 69% more likely to be diagnosed with ADHD and 73% more likely to be medicated compared to the oldest female children in the same grade. According to the study, "The potential harms of overdiagnosis and overprescribing and the lack of an objective test for ADHD strongly suggest caution be taken in assessing children for this disorder and providing treatment."
Iceland, 2012 (Medication Only) - Zoëga et al. "Age, Academic Performance, and Stimulant Prescribing for ADHD: A Nationwide Cohort Study" Although this study did not include statistics on ADHD diagnoses or monthly statistics, it's findings for ADHD medication in children are consistent with other studies. The study reviewed data from 11,785 Icelandic children at ages 9 and 12. Male children born 1-4 months prior to the grade cutoff date were 52% more likely to be medicated for ADHD compared to the oldest male children in the same grade. Female children born 1-4 months prior to the grade cutoff date were 73% more likely to be medicated for ADHD compared to the oldest female children in the same grade. The study concluded that, “Relative age among classmates affects children’s…risk of being prescribed stimulants for ADHD.” (Note: Data from this study was approximated from graphics included in the published version.)
USA, 2010 (Elder) - Elder, "The Importance of Relative Standards in ADHD Diagnoses: Evidence Based on Exact Birth Dates" Of all the studies reviewed, this study from the USA shows the highest increase in risk for diagnosis and medication of ADHD for the youngest children in a class. The study utilized data from 11,784 children in the Early Childhood Longitudinal Study-Kindergarten longitudinal survey that tracked kindergartners in the fall of the 1998–1999 school year through the next nine years. Children born 1 month prior to the September 1st class grade cutoff date were 122% more likely to be diagnosed with ADHD and 137% more likely to be medicated for ADHD. The study concludes by noting a point applicable to all included studies, "Whether relatively young children are overdiagnosed, relatively old children are underdiagnosed, or both, current efforts to define and diagnose ADHD evidently fall short of an objective standard." (Note: Data from this study was approximated from graphics included in the published version.)
USA, 2010 (Evans) - Evans, et al. "Measuring Inappropriate Medical Diagnosis and Treatment in Survey Data: The Case of ADHD among School-Age Children" This study used a sample of 35,343 children from the National Health Interview Survey and 18,559 children from the Medical Expenditures Panel Survey. Children born 1-3 months prior to the grade cutoff date were 27% more likely to be diagnosed for ADHD and 24% more likely to be medicated for ADHD compared to children born 10-12 months prior to the grade cutoff data. The study does a nice job of relating its findings to the "real world" scale of the problem when it states, "To put our estimates into perspective, an excess of 2 percentage points implies that approximately 1.1 million children received an inappropriate diagnosis and over 800,000 received stimulant medication due only to relative maturity."
COUNTER EVIDENCE
In this post we concentrated on studies that have been consistently finding evidence of increased risk of ADHD in the youngest children in a class as evidence for the misdiagnosis and potential over-medication of this population. However, a 2014 Danish study, Pottegard et al. "Children’s relative age in class and use of medication for ADHD: a Danish Nationwide Study" did not support these findings. Although the authors had hypothesized that they would find results consistent with those of other international studies, this did not prove to be the case. In explaining the difference, the researchers postulate, "...that this may be due to the high proportion of relatively young children held back by 1 year in the Danish school system and/or a generally low prevalence of ADHD medication use in the country."
ADVICE FOR PARENTS
Although many of these studies urge "caution" in diagnosing and medicating children for ADHD, they do not provide prescriptive advice to parents. However, using the evidence, it is possible to begin to construct a road map for parents challenged by a child that may have ADHD.
Consider the Age of Your Child - Is your child one of the youngest children in his/her class? If so, is his/her behavior outside the norm for not just his/her grade level, but for kids of his/her specific age? Consider a school with a class cutoff date of September 1st. A child born on August 31st will be in the same class as children born on September 2nd, but will be nearly an entire year younger. This may not seem like a big difference to an adult, but for seven and eight-year-olds, the oldest children in the class will have had a 14% longer life compared to the youngest children in the class. This is no small amount in the context of rapid development in young children and behavior expectations in schools.
Weigh Behavior Outside of School - Is your child also experiencing problems in the home or at play? Do problems seem to manifest in the school disproportionately to other environments? As recommended by the Canadian paper included above, "Greater emphasis on a child’s behavior outside of school may be warranted when assessing children for ADHD to lessen the risk of inappropriate diagnosis." This increases the likelihood that the child's behavior will be based on its own merits and not relative to students that may have a significant age advantage.
Consider Holding a Young Child Back a Year - The possibility that "the high proportion of relatively young children held back by 1 year in the Danish school system" is one of the reasons that the Danish study did not find results consistent with other countries is very intriguing. Parents should carefully consider this option if they suspect that some of a child's school behavior issues may be due to immaturity relative to other classmates.